

Newsletter April 2013
PROJECTS
Data management at ICRH Kenya
The ICRHK data management team is working to improve models used in developing data standards.
 Data management is a vital cross-functional vehicle in clinical trials. ICRH Kenya is sharing knowledge and giving technical support to other clinical data managers from both developed and developing countries. In 2011, the data management unit provided technical support for an ITM study where it was involved in the design and validation of the Pentamidine study database. Through ADMIT (Association of Data Management in the Tropics) ICRH Kenya was also involved in writing data management SOP templates which will be shared with clinical research organizations in the ICRH network. The unit is currently working on a web based Data tracking system with an overall goal of keeping track of the data management process. When completed the system will:
Data management is a vital cross-functional vehicle in clinical trials. ICRH Kenya is sharing knowledge and giving technical support to other clinical data managers from both developed and developing countries. In 2011, the data management unit provided technical support for an ITM study where it was involved in the design and validation of the Pentamidine study database. Through ADMIT (Association of Data Management in the Tropics) ICRH Kenya was also involved in writing data management SOP templates which will be shared with clinical research organizations in the ICRH network. The unit is currently working on a web based Data tracking system with an overall goal of keeping track of the data management process. When completed the system will:
- Support and make more efficient the entire data management process
- Support data cleaning efforts
- Provide data managers with easy access to and information on pages, data and discrepancies interchangeably.
- Assist in quality control audits of CRF data.
This will improve the DM process and it will be available for share to other research organizations.
For more info: contact Mary.Thiong@icrhk.org
HPV vaccinations in Kenya
GAVI funds vaccines to protect girls against cervical cancer in 8 developing countries, among which Kenya.
The human papillomavirus (HPV) is identified as the causal agent behind cervical cancer. Persistent infection with the virus, might lead to the development of cervical abnormalities, and eventually also to cancer of the cervix. The majority of the cases of cervical cancer and related deaths can be found in developing countries (over 85% of all cases). Main factor is the lack of screening and treatment options in low-resource settings.
 Cervical cancer is essentially a preventable disease, and different lines of prevention are available: Primary prevention through HPV vaccination, and secondary prevention through regular screening (i.e. pap smear). Both prevention strategies are virtually lacking in developing countries; the HPV vaccine is too expensive and it is estimated that less than 5% of the women in developing countries has been screened.
Cervical cancer is essentially a preventable disease, and different lines of prevention are available: Primary prevention through HPV vaccination, and secondary prevention through regular screening (i.e. pap smear). Both prevention strategies are virtually lacking in developing countries; the HPV vaccine is too expensive and it is estimated that less than 5% of the women in developing countries has been screened.
Under impulse of dr. Hillary Mabeya (PhD student ICRH), an application for free vaccines was successfully submitted to the Global Access Program of Merck USA. In total, 9600 doses were awarded, sufficient to protect 3200 girls. However, reaching those girls and creating the awareness about cervical cancer and HPV vaccination was still to be done. Therefore, with assistance of ICRH Belgium (dra. Heleen Vermandere), and within the framework of the VLIR IUC Moi University (dr. Davy Vanden Broeck, dr. Violet Naanyu), the necessary efforts were made to successfully distribute the vaccines.
Unfortunately, so many girls remained not vaccinated due to the lack of doses at affordable prices. Under impulse of dr. Hillary Mabeya, the Kenyan government applied for support of the Global Alliance for Vaccine Initiatives (GAVI). GAVI had stated earlier to consider taking HPV vaccines as one of the supported vaccines, and recently it was announced that 8 countries were selected for subsidized HPV vaccines, Kenya being one of those 8 countries.
The demonstration project done in the Eldoret region has been a strong argument in the decision making process to select Kenya as one of the beneficiaries for GAVI funding of HPV vaccines. Partners in this project were: ICRH Belgium, VLIR IUC, Moi University Teaching and Referral Hospital, Eldoret (MTRH), Global Access Program (Axios, Merck USA), MOH Kenya.
More information: Davy.vandenbroeck@ugent.be
 MOMI meeting in Mozambique
MOMI meeting in Mozambique
From March 12th to 14th, the third MOMI (Missed Opportunities in Maternal and Infant Health) Project Management Team meeting took place in Maputo, Mozambique.
Participants included representatives of all the project implementing partners, namely the Institut de Recherche en Sciences de la Sante from Burkina Faso, ICRH Kenya, the Parent and Child Health Initiative from Malawi, ICRH Mozambique, Universidade Eduardo Mondlane from Mozambique, University of Porto from Portugal, University College London from the United Kingdom, and ICRH Belgium.
The opening session was attended by representatives of the Mozambican Ministry of Health, the EC delegation, and the Rector of the Universidade Eduardo Mondlane. During this session an introduction was given of the MOMI project and the consortium, a brief presentation was made of the maternal and infant health situation in the four African project countries, the objectives of the meeting were outlined, and an overview was given of the causes of maternal and infant health in Mozambique and the Ministry of Health goals to reverse maternal and child mortality and improve service coverage rates by 2015. The relevance of MOMI research for enhancing postpartum policies and procedures were highlighted.
During the technical meetings, an overview was given of progress made on the different work packages during the project’s second year of implementation, including the challenges met and lessons learned. A more detailed discussion  followed on the selected interventions that will be implemented in the four countries during the coming year. As such, an agreement was reached on the implementation plan to be followed for the next year.
followed on the selected interventions that will be implemented in the four countries during the coming year. As such, an agreement was reached on the implementation plan to be followed for the next year.
On the final day, the MOMI team visited a primary health care facility, located in Maputo, and discussed maternal and infant services with the director, the chief nurse and the nurse responsible for maternal and infant health services.
DIFFER consortium meeting in South Africa
From February 18th to 22nd, the partners of the DIFFER project met in Durban, South Africa.
 The DIFFER project aims at improving sexual and reproductive health for all women and particularly female sex workers in India, Kenya, Mozambique and South Africa.
The DIFFER project aims at improving sexual and reproductive health for all women and particularly female sex workers in India, Kenya, Mozambique and South Africa.
The objective of this meeting was to share results of the work undertaken by the partner organizations in the first 18 months of the project. The workshop consisted of three days where all partners had the occasion to present data and debate through presentations, group works, and discussions. Participants were also offered the possibility to visit hot spot sites with peer educators as well as a clinic offering sexual and reproductive health services.
Based on those results, the DIFFER consortium is now at work to design the future interventions to start during Fall 2013. DIFFER aims at providing a generic frame for these interventions while ensuring at the same time that the specific context of the four sites is taken into account. The next meeting of the DIFFER consortium will take place in Mysore, India, in November 2013.
Project website: http://differproject.eu
EVENTS
ICRH Belgium lectures
In May 2013 ICRH Belgium will organize two lectures one on ‘Adolescents and sexuality’ and another on ‘violence throughout life’.
The lectures are aimed at a broad target audience of students, researchers, people from NGOs and policy makers.
On May 23th ICRH, Sensoa and Plan Belgium will give a lecture on ‘adolescents and sexuality’. Each organization will shed a light on the topic from their own perspective. Statistics, video testimonies, frameworks and good practices on improvement of adolescents ´sexuality will be presented.
The lecture on ‘violence throughout life’ will take place on May 28th. Various academic and clinical experts will give an overview of experiences of (vulnerability to) violence at different stages of life and how this may be interconnected: as a child, as an adolescent, as an adult and as an elder person.
Both lectures will take place in Ghent (Vredeshuis) and are held in Dutch.
For more information: SaraA.demeyer@ugent.be (adolescents) and Ines.keygnaert@ugent.be (violence throughout life). + LINK TO WEBSITE & REGISTRATION FORM.
ICRH PEOPLE
Two new ICRH professors
On 1 February 2013, Wim Delva and Davy Vanden Broeck were appointed professors at ICRH/Ghent University.
 Prof. Davy Vanden Broeck holds a PhD in molecular biology, and has been working with ICRH since 2008. He is specialized in HPV/cervical cancer, with a special interest in resource poor settings. In addition to his research work in Belgium, he has worked a lot in Kenya, where he still has a teaching assignment at the University of Nairobi.
Prof. Davy Vanden Broeck holds a PhD in molecular biology, and has been working with ICRH since 2008. He is specialized in HPV/cervical cancer, with a special interest in resource poor settings. In addition to his research work in Belgium, he has worked a lot in Kenya, where he still has a teaching assignment at the University of Nairobi.
 Prof. Wim Delva is a medical doctor who has been working for ICRH since July 2006. He graduated as a PhD in 2010, with a thesis on statistical and epidemiological modelling application with regards to sexual behaviour and the spread of HIV. In addition to his work for ICRH, he is senior researcher and deputy director of the South African Centre for Epidemiological Modelling and Analysis (SACEMA) of the Stellenbosch University in South Africa. Both appointments are part-time (10%).
Prof. Wim Delva is a medical doctor who has been working for ICRH since July 2006. He graduated as a PhD in 2010, with a thesis on statistical and epidemiological modelling application with regards to sexual behaviour and the spread of HIV. In addition to his work for ICRH, he is senior researcher and deputy director of the South African Centre for Epidemiological Modelling and Analysis (SACEMA) of the Stellenbosch University in South Africa. Both appointments are part-time (10%).
More information: davy.vandenbroeck@ugent.be and wim.delva@ugent.be
Bavo leaves ICRH
After having worked for ICRH for more than 2 years, Bavo Verpoest leaves the organisation and pursues a career in education.
 Bavo started working for ICRH at the end of 2010. After having assisted the team with several administrative and logistic tasks, he became project assistant in the SEHIB project (Surveillance of HPV infections and HPV related disease subsequent to the introduction of HPV vaccination in Belgium). He was also responsible for compliance with bibliographical procedures. Bavo, a historian by training background, is about to graduate from a pedagogical training, after which he will start a new career as a high school teacher.
Bavo started working for ICRH at the end of 2010. After having assisted the team with several administrative and logistic tasks, he became project assistant in the SEHIB project (Surveillance of HPV infections and HPV related disease subsequent to the introduction of HPV vaccination in Belgium). He was also responsible for compliance with bibliographical procedures. Bavo, a historian by training background, is about to graduate from a pedagogical training, after which he will start a new career as a high school teacher.
More information: bavo.verpoest@ugent.be
Stéphanie De Maesschalck has left ICRH
Stéphanie has been working for ICRH since October 2011 on the CERCA project.
 Stéphanie is a family physician who obtained in 2012 her Phd degree on the physician-patient relationship with ethnic minority patients. Within the context of the CERCA project (Community-Embedded Reproductive health Care for Adolescents in Latin America) she was responsible for communication skills training sessions for healthcare providers working in health centers in Cuenca, Managua and Cochabamba. Stephanie did this with a lot of enthusiasm and will be missed at ICRH. She will continue to work as a family physician in a state refugee centre (Fedasil) and from October 2014 on she will retake her teaching activities on communication skills and cultural competences to medical students at the department of Family Medicine and Primary Health Care, Ghent University.
Stéphanie is a family physician who obtained in 2012 her Phd degree on the physician-patient relationship with ethnic minority patients. Within the context of the CERCA project (Community-Embedded Reproductive health Care for Adolescents in Latin America) she was responsible for communication skills training sessions for healthcare providers working in health centers in Cuenca, Managua and Cochabamba. Stephanie did this with a lot of enthusiasm and will be missed at ICRH. She will continue to work as a family physician in a state refugee centre (Fedasil) and from October 2014 on she will retake her teaching activities on communication skills and cultural competences to medical students at the department of Family Medicine and Primary Health Care, Ghent University.
More information: Stephanie.demaesschalck@ugent.be
Laurence Hendrickx leaves ICRH Belgium (but stays in Mozambique…)
On March 31, Laurence finalized her 5 years mandate as ‘permanent expert’ for the DESAFIO programme at the Eduardo Mondlane University in Maputo, Mozambique.
DESAFIO is the name of an Institutional University Cooperation programme, in which all Flemish universities support the Eduardo Mondlane university by setting up joint research projects, promoting PhD students, organizing courses etc. Laurence was based in Maputo where she was responsible for supporting and facilitating the cooperation. In this capacity, she contributed greatly to the functioning of the programme. Unfortunately, the second five-years stage of the DESAFIO programme, which has started on 1 April 2013, does not provide funding for this position, and it was with regret that we had to let Laurence go.
Besides her work for DESAFIO, Laurence has always been very committed to the work of ICRH in Mozambique. It is thanks to her that ICRH Mozambique could be established as an  autonomous research organization in 2009. In her spare time, Laurence is Administrator and Board of ICRH Mozambique since its establishment, and she will continue this work also in the future.
autonomous research organization in 2009. In her spare time, Laurence is Administrator and Board of ICRH Mozambique since its establishment, and she will continue this work also in the future.
More information: laumozam@gmail.com
‘Mozambique’Laurence has been working for the DESAFIO programme since the start of it, in 2008. tays Administrator of ICRH Mozambique
PUBLICATIONS
Sexual violence against sub-Saharan transmigrants in Morocco
This publication presents the results of a study of knowledge, attitudes and practices of health care workers with regards to the prevention of sexual violence against sub-Saharan transmigrants in Morocco.
Sub-Saharan transmigrants in Morocco are extremely vulnerable to sexual violence. From a public
health perspective, the healthcare system is globally considered an important partner in the prevention of sexual violence. The aim of this study is twofold. In a first phase, it aimed to identify the current role and position of the Moroccan healthcare sector in the prevention of sexual violence against sub-Saharan transmigrants. In a second phase, the researchers wanted these results and available guidelines to be the topic of a participatory process with local stakeholders in order to formulate recommendations for a more desirable prevention of sexual violence against sub-Saharan transmigrants by the Moroccan healthcare sector.
Knowledge, attitudes and practices of healthcare workers in Morocco concerning sexual violence against sub-Saharan transmigrants and its prevention were firstly explored in semi-structured interviews after which they were discussed in a participatory process resulting in the formulation of recommendations. All participants (n=24) acknowledged the need for desirable prevention of sexual violence against transmigrants. Furthermore, important barriers in tertiary prevention practices, i.e. psychosocial and judicial referral and long-term follow-up, and in secondary prevention attitudes, i.e. active identification of victims were identified. Moreover, existing services for Moroccan victims of sexual violence currently do not address the sub-Saharan population. Thus, transmigrants are bound to rely on the aid of civil society.
The authors conclude that their research demonstrates the low accessibility of existing Moroccan services for sub-Saharan migrants. In particular, prevention initiatives addressing sexual violence against the sub-Saharan transmigrant population are absent. Although healthcare workers wish to develop prevention initiatives, they are dealing with structural difficulties and lack of expertise. Recommendations adapted to the context of sub-Saharan transmigrants in Morocco are suggested.
Seline van den Ameele, Ines Keygnaert, Alima Rachidi, Kristien Roelens and Marleen Temmerman.
The role of the healthcare sector in the prevention of sexual violence against sub-Saharan transmigrants in Morocco: a study of knowledge, attitudes and practices of healthcare workers. BMC Health Services Research 2013, 13:77.
Link to full article: http://www.biomedcentral.com/1472-6963/13/77
Quality of antenatal and childbirth care in rural health facilities in sub-Saharan countries
Results of a study aimed at measuring pre-intervention quality of routine antenatal and childbirth care in rural districts of Burkina Faso, Ghana and Tanzania and to identify shortcomings.
In each country, two adjoining rural districts were selected. Within each district, the researchers randomly sampled 6 primary healthcare facilities. Quality of care was assessed through health facility surveys, direct observation of antenatal and childbirth care, exit interviews and review of patient records.
By and large, quality of antenatal and childbirth care in the six districts was satisfactory, but some critical gaps common to the study sites in all three countries were identified. Counselling and health education practices are poor; laboratory investigations are often not performed; examination and monitoring of mother and newborn during childbirth are inadequate; partographs are not used. Equipment required to provide assisted vaginal deliveries (vacuum extractor or forceps) was absent in all surveyed facilities.
The authors conclude that quality of care in the three study sites can be improved with the available human resources and without major investments. This improvement could reduce maternal and neonatal mortality and morbidity.
E. Duysburgh, W-H. Zhang, M. Ye, A. Williams, S. Massawe, A. Sié, J. Williams, R. Mpembeni, S. Loukanova and M. Temmerman. Quality of antenatal and childbirth care in selected rural health facilities in Burkina Faso, Ghana and Tanzania: similar finding. Trop Med Int Health. 2013 Feb 12. doi: 10.1111/tmi.12076.
Efficient HIV prevention requires accurate identification of individuals with risky sexual behaviour. However, self-reported data from sexual behaviour surveys are prone to social desirability bias.
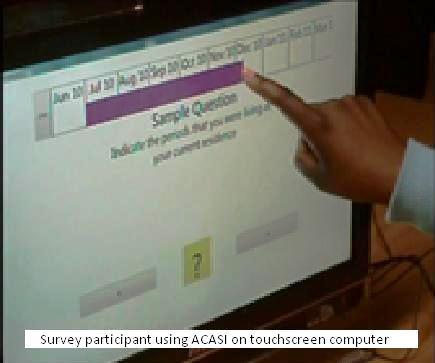 Audio Computer-Assisted Self-Interviewing (ACASI) has been suggested as an alternative to face-to-face interviewing (FTFI), because it may promote interview privacy and reduce SDB. However, little is known about the suitability and accuracy of ACASI in urban communities with high HIV prevalence in South Africa. To test this, we conducted a sexual behaviour survey in Cape Town, South Africa, using ACASI methods. Participants (n=878) answered questions about their sexual relationships on a touch screen computer in a private mobile office. We included questions at the end of the ACASI survey that were used to assess participants’ perceived ease of use, privacy, and truthfulness. Univariate logistic regression models, supported by multivariate models, were applied to identify groups of people who had adverse interviewing experiences. Further, we constructed male-female ratios of self-reported sexual behaviours as indicators of SDB. We used these indicators to compare SDB in our survey and in recent FTFI-based Demographic and Health Surveys (DHSs) from Lesotho, Swaziland, and Zimbabwe. Most participants found our methods easy to use (85.9%), perceived privacy (96.3%) and preferred ACASI to other modes of inquiry (82.5%) when reporting on sexual behaviours. Unemployed participants and those in the 40-70 year old age group were the least likely to find our methods easy to use. In our survey, the male-female ratio for reporting >2 sexual partners in the past year, a concurrent relationship in the past year, and >2 sexual partners in a lifetime was 3.4, 2.6, and 1.2, respectively— far lower than the ratios observed in the Demographic and Health Surveys. Our analysis suggests that most participants in our survey found the ACASI modality to be acceptable, private, and user-friendly. Moreover, our results indicate lower SDB than in FTFI techniques. Targeting older and unemployed participants for ACASI training prior to taking the survey may help to improve their perception of ease and privacy.
Audio Computer-Assisted Self-Interviewing (ACASI) has been suggested as an alternative to face-to-face interviewing (FTFI), because it may promote interview privacy and reduce SDB. However, little is known about the suitability and accuracy of ACASI in urban communities with high HIV prevalence in South Africa. To test this, we conducted a sexual behaviour survey in Cape Town, South Africa, using ACASI methods. Participants (n=878) answered questions about their sexual relationships on a touch screen computer in a private mobile office. We included questions at the end of the ACASI survey that were used to assess participants’ perceived ease of use, privacy, and truthfulness. Univariate logistic regression models, supported by multivariate models, were applied to identify groups of people who had adverse interviewing experiences. Further, we constructed male-female ratios of self-reported sexual behaviours as indicators of SDB. We used these indicators to compare SDB in our survey and in recent FTFI-based Demographic and Health Surveys (DHSs) from Lesotho, Swaziland, and Zimbabwe. Most participants found our methods easy to use (85.9%), perceived privacy (96.3%) and preferred ACASI to other modes of inquiry (82.5%) when reporting on sexual behaviours. Unemployed participants and those in the 40-70 year old age group were the least likely to find our methods easy to use. In our survey, the male-female ratio for reporting >2 sexual partners in the past year, a concurrent relationship in the past year, and >2 sexual partners in a lifetime was 3.4, 2.6, and 1.2, respectively— far lower than the ratios observed in the Demographic and Health Surveys. Our analysis suggests that most participants in our survey found the ACASI modality to be acceptable, private, and user-friendly. Moreover, our results indicate lower SDB than in FTFI techniques. Targeting older and unemployed participants for ACASI training prior to taking the survey may help to improve their perception of ease and privacy.
Beauclair R, Meng F, Deprez N, Temmerman M, Welte A, Hens N, et al. Evaluating Audio Computer
Assisted Self-Interviews in Urban South African Communities: Evidence for Good Suitability and Reduced Social Desirability Bias of a Cross-sectional Survey on Sexual Behaviour. BMC Medical Research Methodology. 2013;13(11).
Link to full article: http://www.biomedcentral.com/content/pdf/1471-2288-13-11.pdf